
National Hemophilia Foundation (NHF) - Posters
Supporting patient voice to inform healthcare decision-making: a discrete choice experiment on disability paradox in hemophilia |
|
|
|
|
OBJECTIVES:
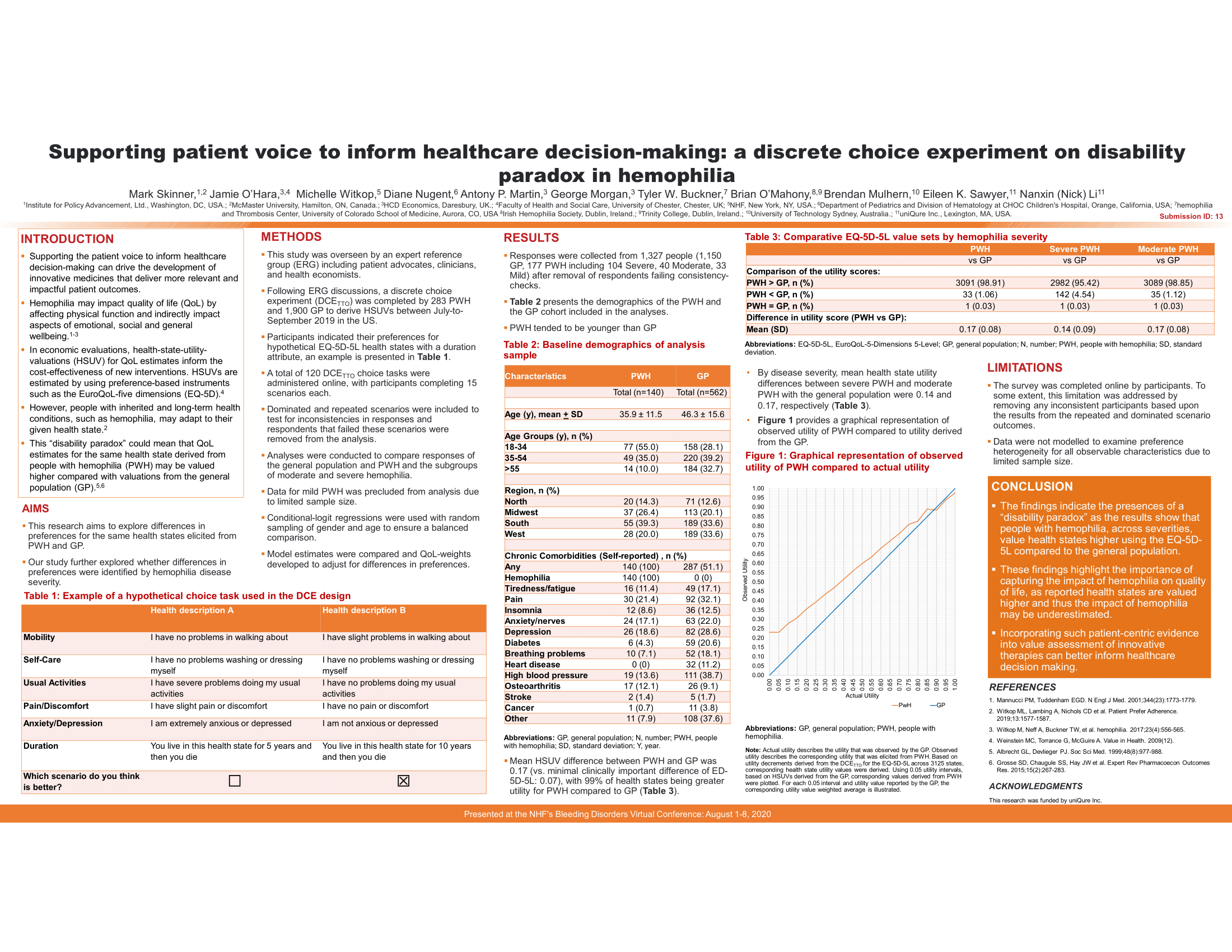
Supporting patient invoice to inform healthcare decision-making can drive the development of innovative medicines that deliver more relevant and impactful patient outcomes. In value assessment of innovative medicines, quality of life (QoL) impact is measured using health state utility valuation (HSUV). However, people with inherited and long-term health conditions such as hemophilia may adapt to their given health state (i.e., the "disability paradox"). Therefore, HSUV estimates for the same health state derived from PWH may be valued higher compared to the general population (GP). As such, this study aimed to explore differences in preferences for the same health states elicited from PWH and GP and whether there were differences in the preferences elicited across hemophilia severity.
METHODS:
This study was overseen by an expert reference group (ERG) including patient advocates, clinicians, and health economists. Following ERG discussion, a discrete choice experiment (DCE) was completed by 283 PWH and 1,900 GP in the US to derive preferences. Participants indicated their preferences for hypothetical EQ-5D-5L health states with a duration attribute. A total of 120 choice tasks were administered online, with each participant completing 15. Dominated and repeated scenarios were included to test for inconsistencies in responses. Conditional-logit regressions were used with random sampling of GP to match the sample of PWH (based on age and gender) for a balanced comparison. Model estimates were compared and QoL-weights associated with the EQ-5D-5L domains and levels were derived.
SUMMARY:
For the DCE, after removal of respondents failing consistency-checks (for dominated and repeated scenarios), responses were collected from 1,327 people (177 PWH including 104 Severe, 40 Moderate, 33 Mild, 1,150 GP). Matching for age and gender (male-only), mean HSUV difference between PWH and GP was 0.17 (vs. minimal clinically-important difference: 0.07). By disease severity, mean HSUV differences between severe PWH and moderate PWH with GP were 0.13 and 0.17, respectively. Data analysis for mild PWH was precluded due to limited sample size.
CONCLUSIONS:
These findings indicate the presence of "disability paradox" in hemophilia. QoL estimates for the same health states derived from PWH may be valued higher compared to GP, indicating under-estimation of the impact of hemophilia. Incorporating such patient-centric evidence into value assessment of innovative therapies can better inform healthcare decision making.


